





リウマチ関節外科について
欧米においては、整形外科医が関節リウマチ(RA)患者の薬物治療を行うことは無いといっても過言ではありません。整形外科の手術においても、リウマチ症例だけを行うのではなく、変形性関節症(OA)やスポーツ傷害などの症例の中で、リウマチという一つの合併症を併せ持った症例として手術加療が行われております。一方、日本においては、現在でも整形外科医も薬物治療を行い、関節破壊の進行を見張るといったスタイルが存在しており、この点は欧米と全く違ったものです。より高度な薬物の開発とともに、副作用や合併症対策もさらに複雑化しているので、整形外科医が内科的治療と外科的治療双方の全てを賄えることは不可能ですが、整形外科医であるリウマチ関節外科医は、RAの診断・可能な範囲での薬物治療・関節破壊進行予防の見張り・内科との連携(マネジメント)・変形に対する手術加療・リハビリテーション、栄養面、心理面、社会生活面でのトータルマネジメントといった一つ一つのRA症例に対する縦断的な治療に携われることが可能で意義深く、そして貴重な存在であります。実際若手先輩医師の紹介のバナーにもありますように、RA診療において、様々なマネジメントができることが重要かつやりがいがあると、複数のリウマチ関節外科医が述べています。ご興味ある方は是非ご一読ください。
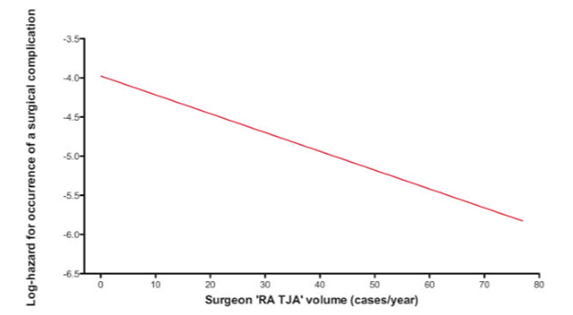
https://www.ryumachi-jp.com/medical-student/lifestyle/
手術においては、最近の傾向としてはRA症例を一つの合併症の1つとしてどこの施設でも手術加療を行ってきた風潮が、RA専門施設に集約されトータルマネジメントの一環の1つの要素として手術が行われるべきとの概念が広まりつつあります。そのためには、最先端のRA外科技術を持った整形外科医師が専門施設においてメスを扱うことが重要になります。普段、リウマチ関節外科医がRA以外の症例もたくさん手術加療を行いながら、たくさんのRA症例を集約的に扱いトレーニングすることがより高度なマネジメントに繋がるのです。次項にも述べますが、リウマチ手術においては、リウマチ症例の手術の経験と術後合併症の頻度が非常に強く逆相関しますので、リウマチ関節外科医は色々な意味で特別なそして貴重な存在という自負を持てるので専門施設での診療・トレーニングに精が出ます。最近ではリウマチ関節外科医は絶滅危惧種??などと呼ばれることもあるようですが、言い方を変えれば、やりがいのある貴重な存在なのです。以下に、例えばリウマチに対する下肢再建手術について各論的に紹介しております。続けて、ご覧ください。
上肢の機能障害に対する手術の考えかた
薬物療法の進歩により手術部位(局所)の炎症は沈静化し、靭帯・腱・関節包などが比較的良好な状態で手術が行われることが多くなりました。そのため、残存した軟部支持組織によるバランス再建術の適応が拡大しています。患者本人も自分の機能障害に気が付かず、長年の変形によって、自分なりに手を使っています。その機能障害や問題に少しでも気づくこと、今何ができないのか、何ができるようになりたいのかを気づかせることが大切です。一方で、機能障害が軽くても外観を気にして手術を希望される患者も増えてきており、第二の顔である手を人前に出せるようになりたいという患者の心情変化が報告されています1)。このようにひとりひとり目標とするところは異なり、それぞれ個別の対応が必要になります。薬物療法だけでなく、手術、リハビリテーション、ケアのトータルマネージメントが重要です(図1)2)。

図1
肩関節障害に対する機能再建手術
肘関節障害に対する機能再建手術

写真1
手関節障害に対する機能再建手術

写真2
Larsen Grade III以上では滑膜切除に加え、尺骨遠位端(尺骨頭)切除11)を行い、関節固定術を追加します。この際、手根骨間関節が残存し尺骨手根骨間関節で手根骨の尺側移動、掌側亜脱臼、回外変形などが見られれば、橈骨月状骨間固定12)を行います(図2)。尺骨手根骨間関節で亜脱臼、脱臼となっている場合には手関節全固定術13,14)が適応となります(図2)。人工手関節全置換術は過去に数多く開発されてきましたが、バランスの不均衡や弛みの問題から長期成績は安定していません。
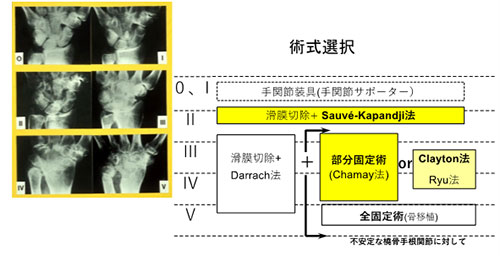
図2
手指関節障害に対する機能再建手術
RA患者の母指はつまみ、握りの動作において、支持性が重要であるため、関節固定術が推奨されます。しかし2関節以上の固定術は、固定による機能障害が大きく、非固定関節の変形を促すことになるため、できるだけ1関節にとどめます。
①ボタン穴変形(boutonnière deformity)
MP滑膜炎が原因となりIP関節過伸展、MP関節屈曲となるもので最も多い母指変形15)です(写真3)。MP関節病変がLarsen Ⅰ, Ⅱの軽度変形例では短、長母指伸筋腱を用いたバランス再建術16)が行われます。さらにGrade Ⅲ, Ⅳではインプラントを用いた関節形成術17)もしくは固定術が行われます。

写真3
2番目に多い変形でCM関節での橈背側への亜脱臼により起こり、第一中手骨が内転しMP関節過伸展、IP関節屈曲となります(写真4)。関節破壊が進行したCM関節には切除関節形成術18)などが行われます。MP関節破壊進行例では関節固定を追加します。

写真4
稀な変形でMP関節の病変によって尺側側副靭帯が弛むことで、基節骨が橈側偏位、中手骨が内転するMP関節橈屈が起こる変形です。関節固定術が適応となります。
④ムチランス変形(mutilating deformity)
動揺関節となったIP、MP関節は、母指長を戻し支持性の獲得のため、関節固定18)を行います(写真5)。

写真5
2) 指関節(示指―小指)
①尺側偏位(ulnar drift)
MP関節で掌尺屈を起こす変形です。術前に徒手矯正ができるか否か(拘縮の有無)で、術後の可動域が変わってきます。変形の早期ではスプリント装着や関節滑膜切除に軟部支持組織によるバランス再建術が行われます。Grade Ⅲ,ⅣではMP関節掌尺側亜脱臼に対しては人工指MP関節置換術20,21)が行われます(写真6)。

写真6
MP関節が屈曲、掌側亜脱臼位をとることで、側索の走行がPIP関節の回転中心の背側を取るようになり、PIP関節過伸展、DIP関節屈曲位となります。治療法は早期ではスプリントが有用です。MP関節が亜脱臼している場合には人工指MP関節置換術による関節再建が行われます。Grade Ⅰ,Ⅱで可動性が有る場合、PIP関節で伸展拘縮解離術と斜支靭帯再建術、Grade Ⅲ, ⅣでPIP関節が強直に近い場合は関節固定を行います。
③ボタン穴変形(boutonnière deformity)
PIP関節の滑膜炎によってPIP関節は屈曲位となり、DIP関節には伸展力が生じます(写真7)。早期では関節滑膜切除を行い、屈曲拘縮例では拘縮解離後、中央索の再建を行います。他動的に伸展ができない場合、屈曲位で関節固定術を行います。人工指PIP関節置換術はPIP関節のアライメント異常がなく変形性関節症性変化がある場合に適応になります。

写真7
参考文献
1. Victoria L et al. Education, self-management, and upper extremity exercise training in people with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res (Hoboken). 66:217-227,2014
2. 山本純己 RA治療の基本的考え方. リウマチ科 27:568-575,2002
3. 公益社団法人日本リウマチ友の会 編2020年リウマチ白書 リウマチ患者の実態(総合編)流 No356,p.25
4. 公益社団法人日本リウマチ友の会 編2020年リウマチ白書 リウマチ患者の実態(総合編)流 No356,p.94
5. Ishikawa H. The latest treatment strategy for the rheumatoid hand deformity. J Orthop Sci 22:583-592,2017
6. Tonga E, et al. Effectiveness of Client-Centered Occupational Therapy in Patients With Rheumatoid Arthritis: Exploratory Randomized Controlled Trial. Arch Rheumatol ;31(1):6-13,2016
7. Sarah E Lamb,et al. Exercises to improve function of the rheumatoid hand (SARAH): a randomized controlled trial. Lancet. 385(9966): 421-429,2015
8. Kojima T, et al. Characteristics of functional impairment in patients with long-standing rheumatoid arthritis based on range of motion of joints: Baseline data from a multicenter prospective observational cohort study to evaluate the effectiveness of joint surgery in the treat-to-target era Mod Rheumatol. 2018 May;28(3):474-481.
9. Kanbe K: Clinical outcome of arthroscopic capsular release for frozen shoulder: essential technical points in 255 patients J Orthop Surg Res. 2018 Mar 16;13(1):56.
10. Ogino H, et al.: Limited extension after linked total elbow arthroplasty in patients with rheumatoid arthritis Mod Rheumatol 2016;26(3):347-51
11. Darrach W Partial excision of lower shaft of ulna for deformity following Colles’ fracture. Ann Surg 57:764-765,1913
12. Chamay A et al. Radiolunate arthrodesis. Factor of stability for the rheumatoid wrist. Ann Chir Main 2:5-17,1983
13. Millender LH et al. Arthrodesis for the rheumatoid wrist. An evaluation of sixty patients and description of a different surgical technique. J Bone Joint Surg 55A:1026-1034,1976
14. 石川肇:リウマチ手関節の治療選択、固定術VS人工関節手術、固定術の立場から. Loco Cure 5:336-341.2019
15. Terrono A et al. Boutonniere rheumatoid thumb deformity. J Hand Surg 15A:999-1003,1990
16. Iwamoto T et al. Modified extensor pollicis longus rerouting technique for boutonnière deformity of the thumb in rheumatoid arthritis. J Hand Surg 41A: e129-134,2016
17. Nemoto T et al. Metacarpophalangeal joint arthroplasty using flexible hinge toe implant with grommets for boutonnière deformity of rheumatoid thumb. J Hand Surg Asian Pac 23:66-70,2018
18. Thompson JS Suspensionplasty. J Orthop Surg Tech 4:1-12,1989
19. Nomura Y et al. Arthrodesis of the digital joint using intraosseous wiring in patients with rheumatoid arthritis. Mod Rheumatol 31:114-118,2021
20. Ishikawa H et al. The effect of activity and type of rheumatoid arthritis on the flexible implant arthroplasty of the metacarpophalangeal joint. J Hand Surg 27B:180-183,2002
21. Gondfarb CA et al. Metacarpophalangeal joint arthroplasty in rheumatoid artritis. A long-term assessment. J Bone Joint Surg 85A:1869-1878, 003
関節リウマチに対する下肢再建手術の意義
はじめに
周術期の注意点
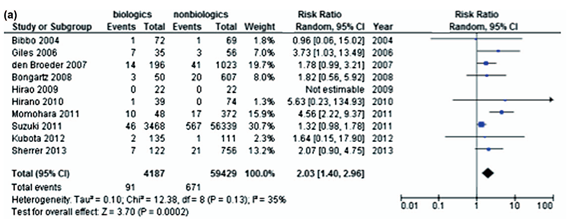
[生物学的製剤使用下での手術後はSSIの頻度が少し上昇する]
各部位におけるRA機能再建手術

股関節障害に対する機能再建手術
膝関節障害に対する機能再建手術
足部障害に対する機能再建手術
後足部・足(距腿)関節
距腿関節の破壊・変形に対しては前述の髄内釘による固定術や、スクリュー固定法、創外固定法などがありますが、可動域減少を回避するためや、対側がすでに固定されているような場合は、TAAも有用な方法の一つです。ただし、非常にメカニカルストレスのかかりやすい部位であるので、インプラントの沈み込みを含んだ弛みを来しやすいと考えておいた方がよいでしょう。そのため、骨粗鬆症治療・骨補強・丁寧な手術計画・正確な骨切り・軟部組織バランスの調整などの注意点が多々あるので、多岐にわたるトレーニングが必要です。人工足関節の種類によっては、一般社団法人日本足の外科学会の主導する新規人工足関節の運用方針(http://www.jssf.jp/medical/leg_prosthesis.html)があり、講習やトレーニングのシステムも存在しているので、是非活用していただければと思います。
中足部
前足部
終わりに
参考文献
1.Lindsay M K Wallace et al. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer’s disease: a cross-sectional analysis of data from the Rush Memory and Aging Project. The Lancet. Neurology. 2019 Feb;18(2);177-184. pii: S1474-4422(18)30371-5.
2.Ito H. et al. Postoperative complications in patients with rheumatoid arthritis using a biological agent – A systematic review and meta-analysis. Mod Rheumatol. 25:672-678,2015
3.Ravi B et al. Increased surgeon experience with rheumatoid arthritis reduces the risk of complications following total joint arthroplasty. Arthritis Rheumatol. 66;488-496,2014
4.WHO Guidelines Approved by the Guidelines Review. Global Guidelines for the Prevention of Surgical Site Infection. Geneva: World Health Organization; 2018
5.日本リウマチ学会(編). 関節リウマチ診療ガイドライン 2014. メディカルビュー社:2014
6.Goodman SM et al. American College of Rheumatology/American Associations of Hip and Knee Surgeons Guidelines for the perioperative Management of Antirheumatic Medication in Patients with Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. J Arthroplasty. 2017;32(9):2628-38
7.伊藤 宣 関節リウマチ周術期における薬物マネジメントのエビデンス 臨床整形外科:患者の満足度を高める関節リウマチ手術, 54(12);1241-1245,2019
8.Hirao M. et al. Laboratory and Febrile Features After Joint Surgery in Patients With Rheumatoid Arthritis Treated With Tocilizumab. Ann Rheum Dis. 68(5):
9.Hirao M. et al. Diagnostic Features of Mild Cellulitis Phlegmon in Patients With Rheumatoid Arthritis Treated With Tocilizumab: A Report of Two Cases. Mod Rheumatol. 21(6):673-7.2011
10.中島 新ほか. 股関節・膝関節の人工関節全置換術. 関節外科:リウマチと整形外科,39(3)66-74,2020
11.小林 秀ほか. 膝の関節リウマチ手術-RAに対するTKAの術後成績、術後満足度について 臨床整形外科:患者の満足度を高める関節リウマチ手術, 54(12);1221-1225,2019
12.Matsumoto T et al. Radiologic Patterning of Joint Damage to the Foot in Rheumatoid Arthritis. Arthritis Care Res (Hoboken). 66(4)499-507;2014
13.Owaki H, Hashimoto J, Hayashida K, Hashimoto H, Ochi T, Yoshikawa H. Short term result of metatarsal realignment for rheumatoid forefoot deformities by metatarsal shortening offset osteotomy. J Bone Joint Surg Br. 2003;85-B, suppl I-80.4
14.Hirao M, Ebina K, Tsuboi H, Nampei A, Kushioka J, Noguchi T, Tsuji S, Owaki H, Hashimoto J, Yoshikawa H. Outcomes of modified metatarsal shortening offset osteotomy for forefoot deformity in patients with rheumatoid arthritis: Short to mid-term follow-up. Mod Rheumatol. 2017 Nov;27(6):981-989.
15.Hirao M, Ebina K, Tsuboi H, Nampei A, Tsuji S, Noguchi T, Owaki H, Hashimoto J. Modified Scarf Osteotomy with Medial Capsular Interposition in Great Toe and Metatarsal Shortening Offset Osteotomy in Lesser Toes for Rheumatoid Deformity. J Bone Joint Surg. Essent Surg Tech. 2018;8(4):p-e7
16.Hanyu T, Yamazaki H, Murasawa A, Tohyama C. Arthroplasty for rheumatoid forefoot deformities by shortening oblique osteotomy. Clin Orthop Relat Res. 1997;338:131-8.
17.Yano K, Ikari K, Iwamoto T, Saito A, Naito Y, Kawakami K, et al. Proximal rotational closing-wedge osteotomy of the first metatarsal in rheumatoid arthritis: clinical and radiographic evaluation of a continuous series of 35 cases. Mod Rheumatol. 2013 Sep;23(5):953-8.
18.Takakubo Y, Takagi M, Tamaki Y, Sasaki A, Nakano H, Orui H, Ogino T. Mid-term results of joint-preserving procedures by a modified Mann method for big toe deformities in rheumatoid patients undergoing forefoot surgeries. Mod Rheumatol. 2010 Apr;20(2):147-53
19.Fukushi J, Nakashima Y, Okazaki K, et al. Outcome of Joint-Preserving Arthroplasty for Rheumatoid Forefoot Deformities. Foot Ankle Int 2016 Mar;37(3):262-8.
20.Niki H, Hirano T, Okada H, Beppu M. Combination joint-preserving surgery for forefoot deformity in patients with rheumatoid arthritis. J Bone Joint Surg Br. 2010;92:380–6.
21.Niki H, Hirano T, Akiyama Y, Mitsui H, Fujiya H. Long-term outcome of joint-preserving surgery by combination metatarsal osteotomies for shortening for forefoot deformity in patients with rheumatoid arthritis. Mod Rheumatol. 2015;25:683-8.
22.Nishida K, Machida T, Horita M, Hashizume K, Nakahara R, Nasu Y, Ohashi H, Saiga K, Ozaki T. Shortening Oblique Osteotomy with Screw Fixation for Correction of the Lesser Metatarsophalangeal Joints of Rheumatoid Forefoot. Acta Med Okayama. 2016 Dec;70(6):477-483.
23.Ebina K, Hirao M, Takagi K, Ueno S, Morimoto T, Matsuoka H, Kitaguchi K, Iwahashi T, Hashimoto J, Yoshikawa H. Comparison of the effects of forefoot joint-preserving arthroplasty and resection-replacement arthroplasty on walking plantar pressure distribution and patient-based outcomes in patients with rheumatoid arthritis. PLoS One. 2017 Aug 29;12(8): e0183805
24.Ebina K, Hirao M, Hashimoto J, Nampei A, Shi k, Tomita T, Futai K, Kunugiza Y, Noguchi T, Yoshikawa H. Comparison of a self-administered foot evaluation questionnaire (SAFE-Q) between joint-preserving arthroplasty and resection-replacement arthroplasty in forefoot surgery for patients with rheumatoid arthritis. Mod Rheumatol. 2017;27(5):795-800.
25.Hirao M, Tsuboi H, Tazaki N, Kushimoto K, Ebina K, Yoshikawa H, Hashimoto J. Effects of range of motion exercise of the metatarsophalangeal joint from 2-weeks after joint-preserving rheumatoid forefoot surgery. Mod Rheumatol. 2019 Mar 29:1-8. doi: 10.1080/14397595.2019.1601853. [Epub ahead of print]
26.Jung HG, Lee DO, Lee SH, Eom JS. Clinical and radiological outcomes of midfoot derotational osteotomy for midfoot-forefoot varus deformity. J Orthop Sci. 2017 May;22(3):468-473. doi: 10.1016/j.jos.2016.12.029. Epub 2017 Mar 21.
27.田中康仁 外反母趾に対する水平骨切り術 整形外科68巻8号;908-913 2017
28.Kushioka J, Hirao M, Tsuboi H, Ebina K, Noguchi T, Nampei A, Tsuji S, Akita S, Hashimoto J, Yoshikawa H. Modified Scarf Osteotomy with Medial Capsule Interposition for Hallux Valgus in Rheumatoid Arthritis: A Study of Cases Including Severe First Metatarsophalangeal Joint Destruction. J Bone Joint Surg Am. 2018 May 2;100(9):765-776
29.Ebina K, Hirao M, Tsuboi H, Kaneshiro S, Nishikawa M, Goshima A, Noguchi T, Nakaya H, Etani Y, Miyama A, Takami K, Hashimoto J, Yoshikawa H. Impact of combining medial capsule interposition with modified scarf osteotomy for hallux valgus. Mod Rheumatol. 2019 Jan 24:1-7. doi: 10.1080/14397595.2019.1572261. [Epub ahead of print]
30.Hirao M, Ebina K, Tsuboi H, Noguchi T, Hashimoto J, Yoshikawa H. Appearance of hindfoot valgus deformity and recurrence of hallux valgus in the very early period after hallux valgus surgery in a poorly controlled rheumatoid arthritis case: A case report. Mod Rheumatol. 2016 Jul 18:1-3.
31.Yamada S, Hirao M, Tsuboi H, Akita S, Matsushita M, Ohshima S, Saeki Y, Hashimoto J. Involvement of valgus hindfoot deformity in hallux valgus deformity in rheumatoid arthritis. Mod Rheumatol. 2014 Sep;24(5):851-4.
32.Cole WH. The treatment of claw foot. J Bone Joint SUrg 1940;22:895-908.
33.Japas LM. Surgical treatment of pes cavus by tarsal v-osteotomy. J Bone Joint Surg [Am] 1968;50:927-44.
34.平尾 眞ほか 下肢の手術の適応と実際② 足部・足関節の手術 関節外科:リウマチと整形外科,39(3)75-79,2020
35.平尾 眞ほか 足趾・足関節の関節リウマチ手術の現状と未来 臨床整形外科:患者の満足度を高める関節リウマチ手術, 54(12);1227-1235,2019
36.Hirao M, Hashimoto, J, Tsuboi, H, Ebina, K, Nampei A, Noguchi T, Tsuji S, Nishimoto N, Yoshikawa H. Total Ankle Arthroplasty for Rheumatoid Arthritis in Japanese Patients: A Retrospective Study of Intermediate to Long-Term Follow-up. J Bone Joint Surg. Open Access. December 28, 2017 – Volume 2 – Issue 4 – p e0033 doi: 10.2106/JBJS.OA.17.00033.
37.Hirao et al. Radiographic Effects Observed in the Coronal View After Medial Malleolar Osteotomy at Total Ankle Arthroplasty in Rheumatoid Arthritis Cases. J Orthop Sci. Feb 13;S0949-2658(20)30011-7. doi: 10.1016/j.jos.2020.01.005. Online ahead of print. 2020